Citation: Dounce SM, Busimi AK, “Optimisation of Syringe Performance for Ocular Injections & Beyond: Impact of silicone Oil”. ONdrugDelivery Magazine, Issue 61 (Oct 2015), pp 27-32.
Susan M Dounce and Anil Kumar Busimi describe the increasingly significant role of prefilled syringes in the delivery of ocular therapeutics.
In recent years, ophthalmic drug delivery has been recognised as having some of the most significantly unmet packaging and delivery needs of any injectable drug market segment. Ocular injections often require very small, precise dose volumes to be administered in a smooth, controlled manner to a precise location in the eye without the introduction of air bubbles or foreign particulate matter such as silicone oil.
The vast majority of these injections are still aseptically prepared from vials into siliconised disposable syringes via a multistep process that can introduce dose inaccuracy, sterility risks, and silicone oil droplets. While these challenges can potentially be addressed by the use of appropriately designed prefilled syringes, such syringes for ocular injections are only newly emerging.
“The high packaging demands of the ophthalmic injectables market are reinforced by the fact that the top two drugs, Lucentis (ranibizumab) and Eylea (aflibercept), which together represented 99% of the 2014 market by revenue and 60% of the market by sales volume, are both biologics…
Of particular concern in ocular injections is the presence of silicone oil droplets and numerous studies have confirmed that silicone oil from disposable syringes is indeed introduced into the eye during injection.1-3 In one study, affected patients were monitored for reactions or complaints of floaters in their fields of vision and while no adverse clinical events were noted, there is general consensus that the situation should be avoided.4 Kocabora et al state, “The functional and clinical consequences of intravitreal silicone oil droplets are unknown, but their occurrence could be avoided by using new-generation prefilled syringes that do not have an internal silicone coating.” 4 Furthermore, studies have shown that low-molecular-weight components of silicone oil can cause acute ocular toxicity in animal models.5
As prefilled syringes begin to gain traction as the preferred delivery mode for ocular injections, silicone oil will be a concern, not only due to the potential for direct complications related to injected droplets, but also from the perspective of safety and efficacy of the drug during long-term storage in contact with siliconised syringe components.1 The high packaging demands of the ophthalmic injectables market are reinforced by the fact that the top two drugs, Lucentis (ranibizumab) and Eylea (aflibercept), which together represented 99% of the 2014 market by revenue and 60% of the market by sales volume, are both biologics. Additionally, the development pipeline for injectable drugs to treat various ophthalmic indications, especially macular degeneration, contains numerous new biologic entities.
The safety and efficacy of biologic drugs can depend sensitively on the exact chemical make-up and three-dimensional conformation of the protein. Interactions with primary packaging can lead to chemical and/ or conformational changes and degradation and/or aggregation, possibly rendering the therapeutic protein ineffective or even immunogenic. The adsorption and desorption of biologics at aqueous-silicone oil interfaces can cause non-native structural conformations to arise and protein aggregates to form.6-7 The nucleation of proteins at silicone oil particle interfaces is a known degradation pathway for some therapeutic biologics and can result in diminished drug efficacy.8 Thus, for ocular injections, in order to minimise complications and to ensure the safety and efficacy of the drugs, the reduction or elimination of free silicone oil is a key value-driver in drug delivery technology development.
Injections into the eye call for a high level of physician control in order to deliver precise doses to precise locations.9 It is therefore desirable for any syringe system used for ocular injections to have a smooth delivery force profile as the drug is being dispensed. However, the overall usability of disposable and prefilled syringes alike is often affected by a stick-slip phenomenon as the syringe plunger traverses areas of the barrel with lower or higher levels of lubrication. During plunger placement and over time as a siliconised plunger is stored in contact with a siliconised syringe barrel, silicone oil can migrate,10 resulting in a non-uniform distribution of lubricant at the plunger’s rest position. This in turn can lead to glide forces that can oscillate from high to low during injection. Stick-slip behaviour is particularly undesirable in precision applications such as ocular injections and reducing or eliminating silicone oil is one way to mitigate this problem.
Prefilled syringes can be designed to address the cleanliness, compatibility, and usability challenges associated with ocular injections but their performance depends on the function of multiple components within the prefilled syringe system. Omniflexcoated plungers, with their lubricious fluoropolymer barrier coating, eliminate the plunger as a source of migrating silicone oil thus enabling long-term compatibility with biologic drugs and highly consistent delivery forces. The syriQ® InJentle syringe, with baked-on silicone, a novel fluid path design, and thin needles, also results in reduced silicone levels, superior compatibility and high-precision drug delivery. Together, OmniflexCP® and the syriQ® InJentle syringe provide an integral solution to the many challenges associated with ocular injections.
DATWYLER OMNIFLEXCP®: LUBRICIOUS, FLUOROPOLYMER BARRIER COATED PLUNGERS

Figure 1: Key differentiators of OmniflexCP®.
Omniflex Coated Plungers (OmniflexCP®) are bromobutyl prefilled syringe plungers with a proprietary, thin, flexible, inert fluoropolymer barrier coating that imparts a low co-efficient of friction without the need for siliconisation (Figure 1). The coating is applied in a twostep process. First, the plungers are loaded into a stainless steel drum and the proprietary fluoropolymer film is applied by a tumble spray coating process. The coated plungers are then subjected to a thermal post-treatment step to covalently bond the coating to the bromobutyl rubber substrate and to form a smooth, continuous fluoropolymer film.
Due to the line-of-sight nature of the spray coating process, the entire plunger surface is coated except for the interior of the plunger-rod cavity. This spray coating process is one of the keys to OmniflexCP®’s superior compatibility and performance. The total coverage of the plunger by the OmniflexCP® spray coating is in contrast to the partial coverage of most film-coated plungers and has the added benefit of providing a complete barrier film on top of every rubber surface that is in contact with the syringe barrel or drug product. The total coverage of the lubricious OmniflexCP® coating also eliminates the need for partial siliconisation of the plunger rills.
The OmniflexCP® coating is designed to reduce extractable levels (especially metal ions) from the base rubber and also to prevent the API or formulation components from interacting with the elastomer.
Omniflex coated closures are widely used throughout the industry for packaging small-molecule drugs that can be absorbed into uncoated elastomers or that may lose potency by reaction with the rubber. The coating is lipophobic / oleophobic and therefore is an excellent barrier for lipidbased or oil-based formulations. In addition to the barrier properties, the lack of siliconisation, very low subvisible particle (SbVP) levels, and highly consistent delivery forces associated with the OmniflexCP® coating make these plungers inherently well suited for biologic drug packaging or for any applications that require high precision drug delivery such as ophthalmic injections.
In a study published in the Journal of Pharmaceutical Sciences, Felsovalyi et al demonstrated that when it comes to silicone oil migrating into a prefilled syringe formulation, the plunger can be the larger source of free silicone as compared with the barrel – even despite the fact that more silicone oil is applied to the barrel.11 Thus, when working to reduce silicone levels and overall SbVP levels from prefilled syringe systems, it is important to consider contributions from both the barrel and from the plunger.

Figure 2: Number of particles greater than 2 µm in size, normalised to 10 cm2 of rubber, for elastomeric closures that have been siliconised with a low viscosity (350 cSt) silicone oil (red bar) versus elastomeric closures that have been Omniflex coated (blue bar). Particle counts are determined in accordance with the method outlined in ISO 8871-3.
Traditionally, elastomeric prefilled syringe plungers are siliconised with a 350- 1000 cSt silicone oil in order to prevent sticking, to enable machinability, and to optimise syringe delivery forces. These low viscosity silicone oils are associated with high levels of SbVPs. Figure 2 shows the number of SbVP’s greater than 2 µm in size per 10 cm2 of rubber surface area for a 350 cSt silicone oil (grey bar) versus an Omniflex coating (blue bar). More than one order of magnitude decrease in SbVP levels is realised for the Omniflex coating compared with siliconisation.

Figure 3: Number of particles per drug contact surface area of a 1 mL long syringe plunger for OmniflexCP®. Particle counts are determined in accordance with the method outlined in ISO 8871-3.
The reason for the significant reduction in particle levels with OmniflexCP® is the absence of silicone oil-based SbVPs. This has been demonstrated by the investigations of Felsovalyi et al. 11 The silicone oil-based SbVP levels of OmniflexCP®, a siliconised plunger, and a film-coated plunger were compared. OmniflexCP® was associated with zero silicone oil-based SbVPs while significant levels detected with the other two plungers. The overall SbVP levels of OmniflexCP® per drug contact surface of a 1 mL long plunger are shown in Figure 3. The lack of siliconisation allows SbVP levels as low as 12 particles / syringe plunger in the range of 2-25 µm (according to ISO standard 8871-3), to be realised.
SCHOTT SYRIQ® INJENTLE – INNOVATIVE STAKED-NEEDLE SYRINGE

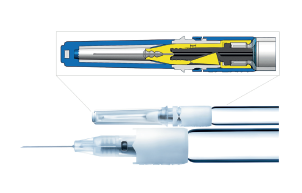
Figure 4: The syriQ® InJentle syringe. The image on the right depicts the elastomer fluid pathway (dark grey) which is also produced by Datwyler. The pinch seal (yellow) is automatically disengaged upon pulling the rigid needle shield to break the tamper-evident ring.
The syriQ™ InJentle prefillable syringe is designed to meet the growing demands of delivery systems for sensitive drugs and safer, more comfortable injections. syriQ® InJentle (Figure 4) consists of a glass barrel and a newly designed syringe cone with a fluid path made of rubber (a component also manufactured by Datwyler), including a staked-in needle. A “pinch seal” keeps the fluid path closed during storage. This newly designed closure prevents the drug from coming into contact with the metal needle or the adhesive. As a result, the drug cannot interact with these substances. The special design of the glass barrel also eliminates the use of a tungsten pin during the glass forming process. Tungsten pins are typically used to keep the fluid path open at the nozzle end of the syringe during the glass forming process. Residual tungsten can migrate into the drug product and lead to unwanted interactions or protein aggregation.
The syriQ® InJentle barrel has baked-on silicone, which significantly reduces the interaction between the drug and the silicone while maintaining syringe functionality. syriQ® InJentle syringes are designed so as to ensure the needle does not stick into the tamper evident needle shield, preserving the needle’s sharpness. This, combined with high-tech needle siliconisation, leads to needles with a low penetration force. In fact, syriQ® InJentle syringes can be offered with thin needles – up to 32 gauge. This makes injections less painful for the patient. syriQ® InJentle includes many special features and offers advantages for ophthalmic injections. This innovative syringe is still delivered in standard nests and tubs and can be filled on standard filling lines.
COMBINED PERFORMANCE OF OMNIFLEXCP® & SYRIQ® INJENTLE SYRINGE SYSTEM

Figure 5: Typical delivery force profiles (100 mm/min) for 1 mL long syriQ® InJentle syringes (29 G, ½” needle) in combination with siliconised plungers (red curve) and OmniflexCP® (blue curve). Syringes were water-filled and aged 105 days at 40°C, 75% R.H. Open circles and squares represent the mean break-loose and glide forces respectively, averaged over 27 samples.
Figure 5 shows typical delivery force profiles (100 mm/min) of the syriQ® InJentle syringe (1 mL long, 29 gauge, ½” needle) in combination with traditional siliconised plungers (red curve) and in combination with OmniflexCP® (blue curve). The syringes, which are lubricated with baked-on silicone, were water-filled and aged at 40°C, 75% relative humidity for 105 days. The siliconised plungers are a standard ISO 1 mL long design, in Datwyler’s FM257 bromobutyl compound (the same base compound as used with OmniflexCP®), siliconised with a 30,000 cSt silicone oil. The open circles and squares in Figure 5 represent the mean break-loose and glide forces, respectively, averaged over 27 samples. These experiments demonstrate that the OmniflexCP® design and the fixed, lubricious Omniflex coating together result in highly consistent forces as compared to siliconised plungers.

Figure 6: Radial stress profiles for ISO designed siliconised plungers (left) versus OmniflexCP® (right) as determined by Finite Element Analysis (FEA).
The Finite Element Analysis (FEA) simulations in Figure 6 (next page) show the impact of the different plunger designs on the radial stress profiles. In the OmniflexCP® design (right) the diameters of the second and third trailing rills have been slightly decreased as compared with the ISO standard (left). Additionally, the trim edge is undercut on the OmniflexCP® design so that it is no longer in contact with the barrel.
Despite the fact that the trim edge is not intended to be a sealing rill, it is a significant contributor to the frictional forces for the ISO standard design. The undercut trim edge and the reduced rill diameters in OmniflexCP® help contribute to the optimum delivery forces in the blue curve in Figure 5.
Beyond the plunger design, the lack of siliconisation of OmniflexCP® is key in eliminating the stick-slip behaviour that is typical of most plungers. Comparing the red and blue curves in Figure 5 it is clear that plunger siliconisation plays a critical role in stick-slip behaviour. Silicone oil distribution, in the region where the plunger and barrel are in contact, has the potential to be non-uniform and change with plunger placement method and storage. For example, when a siliconised elastomeric plunger is compressed in contact with a siliconised syringe barrel, the liquid silicone oil can be squeezed out from between the plunger and barrel.10 This could result in areas of less lubrication on the barrel at the plunger rill / barrel contact points and areas of more lubrication between the plunger rills where the migrating silicone oil has settled. Thus, as it begins to traverse the length of the barrel, the plunger can stick and then slip and has the potential to undergo dynamic axial deformation. This in turn leads to glide forces that can oscillate between high and low. Figure 7 depicts this situation for a traditional siliconised plunger.

Figure 7: Stick-slip behaviour of siliconised plungers. The two images at the top show plunger in storage position (a) and then after all sealing surfaces have completely
passed the initial storage position during injection process (b). Darker grey area on the barrel indicates where there is the high potential for non-uniform silicone oil distribution due to migration during plunger placement and/or storage. Graph below shows typical delivery force profile for a siliconised plunger experiencing a stick-slip behaviour. Average distance between the first and last peak maxima in the graph has a reasonable correlation to the length of the plunger/barrel contact zone.
The two images at the top in Figure 7 show two positions of the plunger in contact with the barrel (grey bar) – first in the storage position (a) and then after all sealing surfaces have completely passed the initial storage position during injection process (b). The darker grey area on the barrel indicates where there is the high potential for non-uniform silicone oil distribution due to migration during plunger placement and/or storage. This region, from the leading rill to the trim edge, has a total length of approximately 6.8 mm as estimated from FEA simulations. This length reasonably correlates to the distance between the first and last peak maxima of the red curves in Figures 5 and 7 (siliconised plungers), which was determined to be 6.6 ± 0.2 mm for 10 curves selected at random. Figure 7a corresponds to the first peak maximum in the graph below, when the plunger movement is first initiated. By the time the plunger has completely passed the initial storage position, as in Figure 7b, the oscillating forces have largely been damped, which would correspond to the displacement beyond the last peak maximum.
Since OmniflexCP® is not siliconised, there is no opportunity for liquid silicone oil from the plunger to be redistributed during plunger placement or during storage. The baked-on silicone of the syriQ® InJentle syringe and the fixed, lubricious OmniflexCP® coating, together result in a significant reduction in stick-slip behaviour and overall, highly consistent delivery forces.
SUMMARY
The combination of OmniflexCP® and the syriQ® InJentle syringe provides an integral solution to the challenges associated with ophthalmic and other precision injection applications. Since OmniflexCP® is not siliconised and since the syriQ® InJentle syringe has many unique features and uses baked-on silicone technology, silicone oil levels are reduced over traditional prefilled syringe systems.
The reduction of silicone levels while maintaining syringe functionality is key to minimising complications after intravitreal injections and helps to ensure superior compatibility with biologic drugs during long-term storage. The OmniflexCP® plunger design and absence of migrating silicone oil enable highly consistent delivery forces without stick-slip behaviour. Smooth glide forces are critical for precision injection applications such as ocular drug delivery as well as for pump-delivery applications.
OmniflexCP® is the leading fluoropolymer barrier coated plunger to provide ultra-low SbVP levels, no siliconisation, highly consistent delivery forces, superior chemical compatibility, and design flexibility.
REFERENCES
- Liu L et al, “Silicone Oil Microdroplets and Protein Aggregates in Repackaged Bevacizumab and Ranibizumab: Effects of Long-term Storage and Product Mishandling”. Invest Ophthalmol Vis Sci, 2011, Vol 52(2), p 1023.
- Bakri SJ, Ekdawi NS, “Intravitreal silicone oil droplets after intravitreal drug injections”. Retina, 2008, Vol 28(7), p 996.
- Freund KB et al, “Silicone oil droplets following intravitreal injection”. Retina, 2006, Vol 26, p 701.
- Kocabora MS et al, “Intravitreal silicone oil droplets following pegaptanib injection”. Acta Ophthalmologica, 2010, Vol 88(2), e44.
- Nakamura et al, “Ocular toxicity of low-molecular-weight components of silicone and fluorosilicone oils”. Invest Ophthalmol Vis Sci, 1991, Vol 32(12), p 3007.
- Jones LS et al, “Silicone Oil-Induced Aggregation of Proteins”. J Pharm Sci, 2005, Vol 94(4), p 918.
- Chantelau EA and Berger M, “Pollution of Insulin with Silicone Oil, A Hazard of Disposable Plastic Syringes”. Lancet, 1985, Vol 1(8443), p 1459.
- Chi EY et al, “Heterogeneous Nucleation-Controlled Particulate Formation of Recombinant Human Platelet- Activating Factor Acetylhydrolase in Pharmaceutical Formulations”. J Pharm Sci, 2005, Vol 94, p 256.
- Sampat KM et al, “Accuracy and Reproducibility of Seven Brands of Small-Volume Syringes Used for Intraocular Drug Delivery”. Ophthalmic Surgery, Lasers & Imaging Retina, 2013, Vol 44(4), p 385.
- Scaraggi M and Persson BNJ, “Time-Dependent Fluid SqueezeOut Between Soft Elastic Solids with Randomly Rough Surfaces”. Tribol Lett, 2012, Vol 47, p 409.
- Felsovalyi F et al, “Silicone-Oil-Based Subvisible Particles: Their Detection, Interactions, and Regulation in Prefilled Container Closure Systems for Biopharmaceuticals”. J Pharm Sci, 2012, Vol 101(12), p 4569.
Previous article
COMPANY SHOWCASE: SPECIALTY COATING SYSTEMSNext article
FLEXIBLE INSPECTION OF PREFILLED SYRINGES