Citation: Oakley T, “Introduction: Device Developer Perspective”. ONdrugDelivery Magazine, Issue 60 (Sep 2015), pp 4-6.
A year on from ONdrugDelivery Magazine’s first wearable bolus (large volume) injectors edition Tom Oakley reviews the need for and state of wearable bolus injectors.
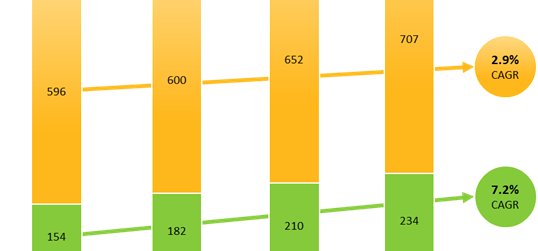
Much has been said and written about the growth in the pharmaceutical industry coming principally from biologics as opposed to small molecules. Research by the Judge Business School of Cambridge University predicts that biologics will enjoy a compound annual growth rate of 7.2%, compared with only 2.9% for small molecules (Figure 1).
If we look at the global sales of existing biologics (Figure 2), we see that the majority are for autoimmune and cancer indications, both of which are dominated by monoclonal antibody-based drugs (mAbs) such as Humira, Remicade, Rituxan, Herceptin and Avastin.
Typically, biologics need to be injected and the most common format is a 1 mL syringe, often prefilled and sometimes in an auto-injector. However, many of the biologics under development require large masses to be injected. In addition, some formulation processes such as PEGylation can increase viscosity. The choice is then whether to use high concentration to fit within 1 mL (which can lead to high viscosity and molecule aggregation) or standard concentration and increase volume above 1 mL. Larger syringes do exist but are avoided due to patient discomfort1 and long injection time.
There are several alternatives to “traditional” syringes and auto-injectors available now or under development. For example:
- Using more than one syringe or auto-injector in series.
- High-pressure auto-injectors such as Oval Medical’s plastic syringe device, which is claimed to deliver drugs at 2,000 cP.
- Needle-free injectors such as Zogenix’ DosePro, which is claimed to deliver drugs up to 1,000 cP.
- Non-spring-powered auto-injectors such as Bespak’s gas-powered Syrina which is claimed to deliver drugs at 200 cP.2
- Wearable bolus (large volume) injectors, which are described later.
Even if the pharmaceutical requirements discussed above were satisfied, there are two other important drivers for developing a new class of devices:

Figure 1: Predicted global pharmaceutical sales volume growth for biologics and small molecules.
- A perception of increasing consumerisation of medical devices, with some patients expecting their medical devices to have the same attractiveness and ease-of-use as their familiar consumer devices. Indeed some patients (and payers) are interested in electronically- enabled and possibly “connected” devices, which could remind and monitor patients and potentially increase adherence (see articles by Unilife and West).
- The need from pharmaceutical companies to differentiate their product and add value relative to innovative competitors, and to biosimilars.
From a device developer’s perspective there is strong and growing demand for new injection devices that deliver large-volume and / or high-viscosity drugs.
We could argue that ambulatory infusion pumps already used for insulin and other drugs could meet the demand, but there are important differences between wearable bolus (large volume) injectors and infusion pumps:
- The injection time in an infusion pump is clinically relevant, whereas for bolus injectors it is as short as patient comfort allows. For example, it may be only a minute or two.
- Many infusion pumps were designed for delivering insulin and cannot deliver the high viscosity biologics described above.
Therefore a need exists for a wearable injector which can deliver high-volume (typically 5 mL but sometimes more) and high-viscosity (many tens of cP) drugs over a few minutes. Such devices are called “bolus injectors” or “large volume delivery devices” or sometimes “patch pumps”.
SURMOUNTABLE CHALLENGES

Figure 2: Biologic drug sales by indication [Source: Bloomberg review of top 13 pharma, 2012].
Commonly used primary packs were not intended, designed or manufactured for use in bolus injectors. The materials (often type 1 borosilicate glass or cyclic olefins) might not be appropriate for the drive mechanisms or shock protection in bolus injectors. Additionally, the form factor of the primary pack used in auto-injectors, pen injectors and some infusion pumps is commonly the 1 mL ‘long’ syringe, or the ‘Lilly type’ 3 mL cartridge, both of which are cylindrical. A bolus injector might desire a flat form because it is attached to the body, so cylindrical primary packs are suboptimal. Pharmaceutical companies tend to be reluctant to use non-standard primary packs due to the large investment in existing infrastructure and knowledge, and the increased risk of any change.
“The injection time in an infusion pump is clinically relevant, whereas for bolus injectors it is as short as patient comfort allows…”
Some devices, like the one from Enable Injections, navigate the primary packaging problem by keeping the drug in a standard vial until immediately before use, at which point the drug is transferred into the bolus injector ready for injection.
In almost all designs, the bolus injector propels the drug formulation from a reservoir into the patient via a thin cannula or needle. These cannulae are subject to pipe-flow physics3 and so, if the cannula must be thin for patient acceptability, the injector must provide a high pressure or accept a long injection time. Any combination of high pressure, long injection time, large delivered volume or high drug viscosity will place force, energy and power requirements on the injector design which are likely to increase size, weight, cost and sometimes technical risks. It is no surprise that device developers have looked beyond the “traditional” spring-powered mechanisms and used novel energy stores. SteadyMed’s expanding battery and Ratio’s expanding hydrogel are two examples.
It is said that, “with great power comes great responsibility”. Indeed, if the injection device is required to provide high pressure, force, energy or power, then there may be challenges to control these during manufacture, storage, use and disposal in a safe way. Sometimes device engineers are pushed down the path of complex mechanical, or electronic, actuators which can have reliability and cost issues.
Some drugs require cold chain transport and storage, which can increase viscosity further (and decrease comfort) if warm-up times are not adhered to. Other drugs need reconstituting from powder form.
Additionally, the intellectual property space is crowded and so freedom to operate is a key issue.
RECENT NEWS AND DEVELOPMENTS
In the past year, we have seen some interesting developments in this area.
On the standards front, ISO 11608-6 “Needle-based injection systems for medical use – requirements and test methods – Part 6: Bolus Injectors”, is making its way through the drafting process.
Examples of the requirements to be clarified in the standard are:
- Method and robustness of the attachment to the body (or perhaps clothes)
- Interaction with the needle or cannula
- Whether IV injection is covered
- Testing (such as shock) whilst delivering drug, which is not required for syringes or auto-injectors.
In the area of partnering, deals that have been made public include the master services agreement for Unilife to supply wearable injectors to Sanofi for 15 years. Another is the development deal between Enable Injections and CSL Behring.4
There have been various other newsworthy developments in the field. Roche received regulatory approval in Europe for the Single Injection Device (formerly MyDose) with Herceptin SC. However, it has not been launched on the market at the time of writing. Bespak has announced its Lapas bolus injector, targeted at the low-cost end of the bolus injector market.5 Ratio Drug Delivery ceased developing its NuPrivo hydrogel-based bolus injector, and BD has renamed its Microinfusor to Libertas (page 30).
Looking forward, we can expect to see continued strong interest from pharma companies in the large volume device sector, and the race to launch the first true bolus injector is still wide open.
REFERENCES
- Jorgensen JT et al, “Pain assessment of subcutaneous injections”. Annals Pharmacother, 1996, Vol 30, pp 729- 732.
- www.bespak.com/Syrina.
- See the Hagen-Poiseuille equation.
- “Interview: Jeannie Joughin, CSL Behring”, ONdrugDelivery Magazine, Issue 55 (Feb 2015), pp 53-55.
- www.bespak.com/Lapas.
Previous article
SELECTING THE RIGHT WEARABLE INJECTOR TECHNOLOGY AND PARTNERNext article
GETTING TO KNOW ENABLE INJECTIONS