

Citation: Varum F, Bravo R, Basit A, “OPTICORE™: a First-in-Class Colonic Targeting Technology”. ONdrugDelivery Magazine, Issue 109 (July 2020), pp 40–44
Felipe Varum, Roberto Bravo, PhD and Abdul Basit discuss the use of colonic targeting coating technology OPTICORE™ to deliver APIs in the treatment of ulcerative colitis (UC) patients.
The large intestine remains a relatively unexplored part of the gastro-intestinal (GI) tract in terms of drug delivery. Despite several physiological challenges that need to be overcome, it offers significant and attractive possibilities for drug product manufacturers. Delaying drug release serves multiple purposes, including protection of acid-labile drugs and protection of the stomach from irritating compounds.
“To allow complete drug release in the colon, accurate targeting and rapid coating dissolution is paramount to ensure effective delivery.”
Moreover, colonic targeting opens new avenues for delivery and systemic absorption of molecules that undergo degradation and/or are poorly absorbed in the upper GI tract.1 This is due to the low levels of luminal and mucosal metabolic enzymes found in the colon, in comparison with the small intestine,2,3 and drugs which are substrates for intestinal cytochrome P450 enzymes (CYPs) and efflux transporters.4,5
Targeting the distal part of the gut relies almost exclusively on enteric coatings (pH-sensitive polymers) based on Eudragit® S100, Eudragit®L100 (Evonik) or mixtures thereof. A range of successful drug products employing enteric coatings are available as first-line treatments for mild-to-moderate inflammatory bowel disease conditions such as UC, Crohn’s disease and microscopic colitis. They include: Asacol™/Octasa®/Asacolon™/Fivasa™ (mesalazine; Tillotts Pharma/Allergan), Mezavant®/Lialda®(mesalazine; Cosmo Pharmaceuticals) and Entocort™ (budesonide, Tillotts Pharma).then gradually increases until the distal small intestine.
However, a luminal pH drop occurs at the ileocaecal junction due to the production of short chain fatty acids by colonic microbiota. This halts the pH increases observed in the small bowel, and results in challenges to the triggering of pH-sensitive dissolution systems in the colon. To allow complete drug release in the colon, accurate targeting and rapid coating dissolution is paramount to ensure effective delivery, even under challenging conditions of rapid transit time and significant pH drop in the colon – as often seen in patients with UC.6
A NOVEL SOLUTION
OPTICORE™ is a first-in-class validated colonic targeting coating technology.7 It comprises two trigger systems (pH and bacterial enzymes) enabled by the incorporation of Intract Pharma’s Phloral® in the outer layer (Figure 1). There is also an inner layer promoting release acceleration.

Figure 1: Schematic representation of OPTICORE™ outer layer release triggers.
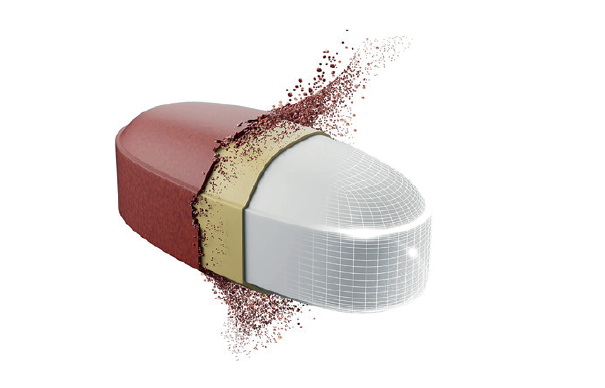
The inner layer of OPTICORE™ builds on the benefits of the Duocoat® technology (Evonik) in accelerating drug release from enteric coated dosage forms.8,9 This layer is composed of a partially neutralised enteric polymer with a buffer salt (Figure 2). The high pH, buffer capacity and ionic strength promotes an active acceleration of the dissolution of the enteric polymer in the outer layer as soon as one of the release triggers is initiated (fail-safe feature).

Figure 2: Schematic representation of the OPTICORE™ coating structure and tablet
disintegration in the colon.7
The presence of the inner layer beneath the outer layer promotes a faster drug release from OPTICORE™ coated tablets (Figure 3) in buffer simulating the luminal composition of the terminal ileum (pH 7.4 Krebs buffer) in comparison with state-of-the art enteric coatings designed for colonic targeting (Eudragit® S, (Evonik) dissolves above pH 7).
The outer layer of OPTICORE™ comprises the two-trigger release technology Phloral®.10,11,12 This combines an enteric polymer, such as Eudragit® S, which is responsible for the pH-driven dissolution, and resistant starch (Figure 2). When embedded into the outer layer coating, this polysaccharide does not dissolve or swell during transit in the upper gut and resists digestion by salivary and pancreatic enzymes.
In the large intestine, where bacterial numbers are several orders of magnitude higher than in the upper gut, resistant starch can serve as a source of energy for colonic microbiota. This allows for weakening of the coating structure, acting as a second drug release trigger, even in conditions of lower luminal colonic pH and fast transit time, as often seen in UC patients.

Figure 3: Drug release from OPTICORE™ coated tablets mediated by pH and by bacterial enzymes.
Below the pH trigger (pH = 7) of the enteric polymer in the outer coating, drug release from OPTICORE™ coated tablets can be initiated due to the action of bacterial enzymes (Figure 3) as shown in a model of the human colon (human faecal slurry).7
The combination of these features provided by the outer and inner layer allows an accurate and timely release of the API in the ileo-colonic region, making it available throughout the colon (Figure 2). The versatility of the OPTICORE™ technology makes it suitable for use in any type of oral solid dosage forms such as tablets, capsules or pellets.
Optionally, an isolation layer between the drug-containing core and the inner layer may be used, particularly if the drug is acidic, which may limit the features of the inner layer in terms of enteric polymer dissolution acceleration.
CLINICAL PROOF OF CONCEPT AND BENEFITS
The benefits of the dual-trigger system (Phloral®) to ensure accurate colonic targeting have been demonstrated in healthy human subjects by means of gammascintigraphy10 and in Clostridium difficile patients who received a faecal material transplantation delivered in capsules coated with this technology.11
“OPTICORE™ coating technology offers significant advantages, particularly for accurate drug delivery in the colon of
UC patients, even when using single unit dosage forms, such as tablets.”
The OPTICORE™ technology has been successfully implemented in a novel mesalazine 1600 mg drug product. Gammascintigraphy investigations showed accurate colonic targeting in all subjects enrolled in the study (Figure 4), allowing for a distribution of the drug along the colon to ensure sufficient local concentrations, both in healthy subjects and in mild-to-moderate UC patients.
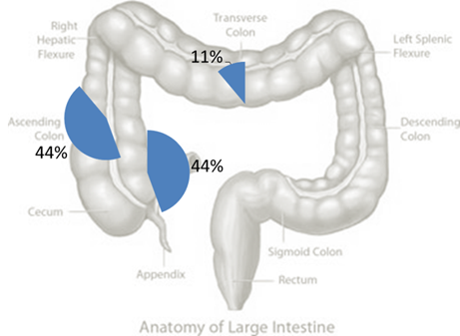
Figure 4: Representation of OPTICORE coated tablets’ disintegration locations within the large intestine in human volunteers (followed by gamma-scintigraphy).
OPTICORE™ coated 1600 mg tablets successfully met the primary clinical endpoints (clinical and endoscopic remission) of the largest mesalazine induction therapy Phase III study incorporating central reading.13 The first drug product developed based on the OPTICORE™ technology is now available from Tillotts Pharma for treating UC patients in multiple markets under the brands Asacol™ 1600, Octasa™ 1600, Yaldigo™ 1600 and Asacolon™ 1600.
CONCLUSIONS
OPTICORE™ coating technology was successfully developed by combining an alkaline inner layer with an outer enteric layer embedded with pH and enzymatic triggers. The inclusion of resistant starch to the Eudragit® S coating formulation does not impact coating robustness and the enteric properties, but is designed to allow an accelerated drug release when the pH of the luminal fluid is above seven (as in Krebs buffer pH 7.4) or below seven (as in pH 6.8 human faecal slurry). Therefore, OPTICORE™ coating technology offers significant advantages, particularly for accurate drug delivery in the colon of UC patients, even when using single-unit dosage forms, such as tablets.
REFERENCES
- Lee SH et al, “Strategic approaches for colon targeted drug delivery”. Pharmaceutics, 2020, Vol 12(1), pp 68.
- Yadav V et al, “Gastrointestinal stability of therapeutic anti-TNF α IgG1 monoclonal antibodies”. Int J Pharm, 2016, Vol 502 (1–2), pp 181–187.
- Bak A et al, “Local delivery of macromolecules to treat diseases associated with the colon”. Adv Drug Deliv Rev, 2018, Vol 136–137, pp 2–27.
- Tubic-Grozdanis M et al, “Pharmacokinetics of the CYP 3A substrate simvastatin following administration of delayed versus immediate release oral dosage forms”. Pharm Res, 2008, Vol 25 (7), pp 1591–1600.
- McConnell EL et al, “Colonic treatments and targets: issues and opportunities”. J Drug Target, 2009, Vol 17 (5), pp 335–363.
- Fallingborg J et al, “Very low intraluminal colonic pH in patients with active ulcerative colitis”. Dig Dis Sci, 1993, Vol 38 (11), pp 1989–1993.
- Varum F et al, “OPTICORE™, an innovative and accurate colonic targeting technology”. Int J Pharm, 2020, Vol 583, pp 119372.
- Liu F et al, “A novel double-coating approach for improved pH-triggered delivery to the ileo-colonic region of the gastrointestinal tract”. Eur J Pharm Biopharm, 2010, Vol 74 (2), pp 311–315.
- Varum F et al, “A novel coating concept for ileo-colonic drug targeting: proof of concept in humans using scintigraphy”. Eur J Pharm Biopharm, 2013, Vol 84 (3), pp 573–577.
- Ibekwe VC et al, “A new concept in colonic drug targeting: a combined pH-responsive and bacterially triggered drug delivery technology”. Aliment Pharmacol Ther, 2008, Vol 28 (7), 911–916.
- Allegretti JR et al, “Fecal microbiota transplantation capsules with targeted colonic versus gastric delivery in recurrent Clostridium difficile Infection: A comparative cohort analysis of high and low dose”. Dig Dis Sci, 2019, Vol 64 (6), pp 1672-1678.
- Varum F et al, “A dual pH and microbiota-triggered coating (PhloralTM) for fail-safe colonic drug release”. Int J Pharm, 2020, Vol 583, pp 119379.
- D’Haens GR et al, “Randomised non-inferiority trial: 1600 mg versus 400 mg tablets of mesalazine for the treatment of mild-to-moderate ulcerative colitis”. Aliment Pharmacol Ther, 2017, Vol 46 (3), pp 292–302.
Previous article
UNIQUE MINITABLET DISPENSER MEETS FLEXIBLE ORAL DOSING NEEDNext article
INTERVIEW WITH MILENA BATALLA, PHD, PANARUM