Citation: Fureby A, Elofsson U, Gerde P, “Pulmonary Delivery of Antimicrobial Peptides”. ONdrugDelivery Magazine, Issue 57 (Apr 2015), pp 4-7.
Anna Fureby, Ulla Elofsson and Per Gerde discuss the serious problem of antibiotic resistance and the potential role of antimicrobial peptides in the treatment of resistant bacterial strains.
Resistance to traditional antibiotics is a rapidly increasing problem that in a few years could make infections impossible to treat and bring the state of medical care back to the pre-antibiotic era from the beginning of the last century. Antimicrobial peptides (AMPs) have a huge potential as new therapeutics against infectious diseases as they are less prone to induce high-level resistance due to their fast and non-specific mechanism of action.
A NEW APPROACH TO BACTERIAL LUNG INFECTION – FORMAMP
“To date, no products based on AMPs have reached the market. One of the main reasons is the challenge related to stability of peptides during storage as well as after administration…”
A large variety of AMPs have been identified and isolated from plants, animals and humans and their structure is well preserved. These have also been assessed, analysed and modified in order to increase their function and efficiency for drug delivery applications. These peptides act by interacting with the bacterial membranes and by perforating the membrane (see Figure 1). However, only a few candidates have reached late stages of clinical trials and, to date, no products based on AMPs have reached the market. One of the main reasons is the challenge related to stability of peptides during storage as well as after administration, which dramatically reduces the efficiency.

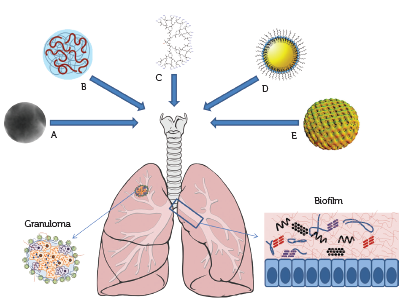
Figure 1: Nanocarriers investigated in FORAMAMP for delivery of antimicrobial peptides to the lungs for treatment of tuberculosis associated with granuloma and cystic fibrosis associated with biofilm.
These challenges are addressed in “FORMAMP – Innovative Nanoformulation of Antimicrobial Peptides to Treat Bacterial Infectious Diseases”, a large collaborative project within EU’s NMP-programme. The aim of FORMAMP is to explore innovative nanoformulation strategies to formulate well-characterised AMP candidates in order to improve the efficiency and stability of the peptides in clinical development. In addition, the nanocarriers are formulated in functional dosage forms, i.e. for pulmonary delivery for local treatment of bacterial infections.
Different nanoformulation platforms, particularly promising for peptide delivery, controlled-release strategies and technologies against proteolytic degradation of peptides will be evaluated in the project. These include carriers of organic origin (lipid-based and polymer-based systems) as well as inorganic carriers (nanostructured silica). The effect of nanoformulated AMPs will be evaluated with state-of-the-art in vitro and in vivo models. The results of this interdisciplinary project will generate efficient treatment strategies combatting one of the largest threats to our healthcare system and society today, reducing healthcare costs and expanding the growth of European enterprises within the field of pharmaceutics and nanomaterials.
TB & CF – DISEASES IN NEED OF NOVEL COMPLEMENTING MEDICATIONS
A wide-spread, but usually curable pulmonary disease is tuberculosis (TB). About 2 billion people are infected by Mycobacterium tuberculosis (MTB) and, in 2012, 8.6 million people developed tuberculosis.1 The bacterium infects when it is inhaled and subsequently reaches the alveoli, where the bacilli are phagocytised and accumulate in alveolar macrophages, the cells form a hard shell (granuloma) that keep the bacilli contained, and can survive in a dormant state for years. If the MTB overcome the immune system of the infected individual, the infection progresses as the bacteria multiply rapidly, so that TB develops. The patient is infectious at this time.
Most cases of TB are pulmonary but it can occur in almost any anatomical site. In recent years, drug-resistant TB has become more widespread, which makes treatment of the disease more complex. Already, drug-sensitive TB requires a treatment period of about six months using different combinations of antibiotics.
“The results of this interdisciplinary project will generate efficient treatment strategies combatting one of the largest threats to our healthcare system and society today…”
Cystic fibrosis (CF) is an autosomal recessive genetic disorder that affects mainly the lungs but also the pancreas, liver, kidneys and intestine. It is caused by the presence of mutations in both copies of the gene for the protein cystic fibrosis transmembrane conductance regulator (CFTR). The production of sweat, digestive fluids and mucus is influenced by CFTR so that the viscosity of these secretions is increased. The disease is most common among people of European ancestry, and affects around 70,000 people worldwide. In Europe, approximately 1 in 3000 newborn infants is diagnosed with CF. The average life expectancy is between 37 and 50 years in the developed world, and the major cause of deaths is lung problems.
A particular problem that occurs in addition to repeated lung infections is the excessive and sticky mucus in the lung and the generation of biofilms that are colonised by different bacteria, such as Pseudomonas aeruginosa, Staphylococcus aureus, and Haemophilus influenza. When located in the biofilm, the bacteria tend to develop antibiotic resistance and also become less available for the drugs, administered orally or by inhalation.
Thus, for both MTB and CF there is a need to find novel treatments that can penetrate into the granuloma or into the biofilm to reach the bacteria and take effect. For both diseases, development of antibiotic-resistant strains of bacteria is a common and increasing problem. Current research addresses this issue by, for example, developing nanoformulations of established active substances to enhance their effect.
As mentioned above, an attractive alternative to conventional small-molecule antibiotics is antimicrobial peptides. In FORMAMP antimicrobial peptides are used that have demonstrated activity towards bacterial strains (including some drug-resistant strains) such as P. aeruginosa, S. aureus and M. tuberculosis, without showing negative effects on human cells. In order to make these available as medications, nanostructured formulations are necessary.
NANOCARRIERS FOR PULMONARY DELIVERY OF PEPTIDES

Figure 2: Schematic illustration of the possible action mechanisms of antimicrobial peptides interacting with cell membranes.13
As soon as they enter the body, AMPs, as well as other peptides and proteins, are attacked by proteases, which break them down into amino acids and shorter fragments. Further, the complicated structures make them sensitive to breakdown during storage where interactions with device surfaces, air/water interfaces, presence of enzymes, may result in loss of the effect. Combining peptides with a (nano)carrier can protect the peptide from the proteolytic attack and also provide prolonged or triggered release. For inhalation therapy, the inhaled particles or droplets need to be in the respirable size range, 1-5 µm, and thus the peptides must be formulated to meet this requirement. The preferred delivery form is inhaled powders, as this enables high drug concentrations and the lengthy inhalation time of nebulisation is circumvented. Dry formulations also bring the advantage of increased storage stability even at room temperature. An additional problem that can be encountered in nebulisation is that the peptides are damaged during the droplet formation. Different nanoformulation platforms, particularly promising for peptide delivery, controlled-release strategies and technologies against proteolytic degradation of peptides will be evaluated in the project. These include lipid-based systems such as lipidic nanocapsules and self-assembled lipid nanoparticles, polymer-based structures such as dendrimers and microgels as well as nanostructured mesoporous silica, schematically illustrated in Figure 2.
The peptides in FORMAMP are new, but peptides for other medical uses have been under investigation for a few decades, as the lung is a suitable route for systemic delivery without first-pass effects.
The most studied peptide for pulmonary delivery is insulin, for which rapid systemic delivery is the target. Such a product was on the market for a short period in 2006/2007. For improved delivery and to avoid phagocytosis insulin was spray-dried as larger very porous particles (Pulmospheres®). Recently, the US FDA approved a new insulin formulation for inhalation that is produced and marketed by MannKind Corporation (Valencia, CA, US) and Sanofi (Paris, France). Insulin is formulated with fumaryl diketopeperazine as the carrier, which self-assembles through hydrogen bonding in mildly acidic environment to form microspheres (Technosphere®).
When addressing tuberculosis via pulmonary delivery, the specific target is the macrophages that carry the MTB inside. Therefore phagocytosis is desired in contrast to e.g. insulin delivery. Literature indicates that infected macrophages have higher phagocytic activity compared with uninfected macrophages, which may be used to improve targeted delivery.2 For efficient uptake in the macrophages the microparticle should have the appropriate size and surface characteristics. The optimal size is about 3 µm (range 1-10 µm).
Nanoformulation concepts used for pulmonary delivery of various small-molecule TB drugs such as rifampicin may be possible to translate to peptide delivery, although this has not been tested yet.
One of the most studied concepts is liposomes, which are able to hold active substances inside as well as in/on the surface of the liposomes. These have mostly been studied in nebulised form with success at least in animal models, but few studies of dried liposomes are available.1 In order to increase their residence time in the lung, liposomes have been modified with, for example, chitosan.3
Alternative nanoparticles for drug delivery are e.g., PLGA particles, alginate-chitosan hybrid particles,5 and hyaluronan particles,6 which all provide longer residence time in the lungs.7,8
In general, studies using animal models have shown that the therapeutic index can be improved and the dose to reach the local MIC can be reduced when nanoformulations are used.
Peptides that attack P. aeruginosa and other species in biofilms associated with CF need to penetrate the matrix of the biofilm. This is composed of polysaccharides and DNA, which both increase the viscosity. Positively charged polymers can help break up the biofilm matrix. Liposomes and PLGA particles have been studied by several groups and, when tested, the antimicrobial efficiency compared with free drug has been enhanced in most cases. It has been shown that the surface charge of liposomes is important for the delivery of the drug, so that positively charged liposomes are more efficient than negatively charged, whereas neutral liposomes do not penetrate the biofilm.9
However, other studies show that neutral liposomes can be efficient in delivering antibiotics in cystic fibrosis biofilms.10 Hybrid particles composed of a PLGA core and a lipid coating has also been investigated with enhanced drug delivery in biofilms.11
The effect of the nanoformulated AMPs in FORMAMP will be evaluated with state-of-the-art in vitro models and in vivo models. These models include macrophage exposure models for anti-TB assessment, and a biofilm model where a controlled biofilm can be grown, evaluated for structural changes and viability after delivery of AMP, and be exposed to labelled particles which are tracked to enable evaluation of the penetration into the biofilm. Initial results from in vitro models are promising and show in most cases that the AMP is preserved and in some cases even improved by the presence of nanoformulations.
Most of the excipients used in nanoformulations are not approved for pulmonary delivery, thus the introduction of these formulations will necessitate regulatory approval. This may constitute a hurdle to the introduction of these novel formulations, but it needs to be overcome to make new and innovative therapies available to the patients in need.
EVALUATION OF POTENTIAL FOR PULMONARY DELIVERY
In order to be efficacious for treating pulmonary diseases, nanoformulated peptides need to be delivered in the right area of the lung. During development of new formulations for pulmonary delivery of peptides it is critical to evaluate these under sufficiently in vivo-like conditions. In creating a carrier aerosol two parameters are of cardinal importance for performance:
- the aerodynamic particles size distribution combined with the ventilation manoeuver will determine the prime region of exposure in the respiratory tract
- the release characteristics of the therapeutic peptides from the carrier formulation will influence the delivery rate of the peptides to the surrounding lung tissues.
To evaluate these properties fully it is of great value if the same aerodynamic aerosol can be delivered to several complementary exposure modules, including the standard cascade impactors for assessment of aerodynamic particle size. To this end the PreciseInhaleTM platform is used,12 consisting of a series of exposure modules from cascade impactors, cultured lung epithelial cells, isolated perfused rodent lungs to tracheally intubated-, or nose-only rodents can be exposed to the very same aerosol formulation throughout.
For soluble peptides there is a rapidly decreasing rate of absorption in the lungs with increasing molecular weight. So for smaller peptides nanoformulations can be used both to decrease the absorption rate in the lungs thereby increasing effect duration, and to protect the peptides from enzymatic degradation in the lungs. The two exposure models most useful for detecting the inhalation pharmacokinetics of the various formulations is the isolated ventilated and perfused lung of the rat (IPL), and the intratracheally intubated rat (IT). The IPL provides a high resolution absorption curve of the peptide into the circulation for up to three hours after exposure. The IPL model can be very useful when comparing the absorption rate of a peptide formulated as neat powder or when incorporated into various more advanced nanoformulations. These exposures should be complemented with intratraecheal exposures to the same formulations revealing the systemic distribution of the inhaled compounds for longer periods after inhalation. A third model that could be of interest for deriving comparative data is by exposing to the same aerosols airway epithelial cells that are cultured at airlifted conditions in Transwell inserts and perfused in single-pass mode. This could derive valuable data from a 3R (replacement, reduction and refinement) standpoint.
CONCLUSION
In summary, novel nanoformulations have been shown to be promising for the delivery of small-molecule antibiotics to treat both tuberculosis and cystic fibrosis. A particular advantage is the possibility for local drug delivery in the lung. The extension of using similar nanoformulation platforms for delivery of antimicrobial peptides holds promise for the future and is currently under development in FORMAMP. The development of such novel formulations will necessitate regulatory approval of excipients new to pulmonary delivery as well as of the antimicrobial peptides.
ACKNOWLEDGMENT
The research leading to these results has received funding from the people of the European Union via the EU Seventh Framework Programme ([FP7/2007-2013]) under grant agreement No. 604182.
It was carried out within the project FORMAMP – Innovative Nanoformulation of Antimicrobial Peptides to Treat Bacterial Infectious Diseases.
REFERENCES
- Kaur IP, Singh H, “Nanostructured drug delivery for better management of tuberculosis”. J Controlled Release, 2014, Vol 184, pp36-50.
- Hirota K, Tomoda K, Inagawa H, Kohchi H, Soma G, Makino K, “Stimulation of phagocytic activity of alveolar macrophages toward artificial microspheres by infection with mycobacteria”. Pharm Res, 2008, Vol 25, p 1420-1430.
- Changsan N, Chan HK, Separovic F, Srichana T, “Physicochemical characterization and stability of rifampicin liposome dry powder formulations for inhalation” J Pharm Sci, 2009, Vol 98, pp 628-639.
- Zaru M, Manca ML, Fadda AM, Antimisiaris SG, “Chitosan-coated liposomes for delivery to lungs by nebulization”. Colloids Surf B Biointerfaces, 2009, Vol 71, pp 88-95.
- Zahoor A, Sharma S, Khuller G, “Inhalable alginate nanoparticles as antitubercular drug carriers against experimental tuberculosis”. Int J Antimicrob Agents, 2005, Vol 26, pp 298-303.
- Hwang SM, Kim DD, Chung SJ, Shim CK, “Delivery of ofloxacin to the lung and alveolarmacrophages via hyaluronanmicrospheres for the treatment of tuberculosis”. J Controlled Release, 2008, Vol 129, pp 100–106.
- Suarez S, O’Hara P, Kazantseva M, Newcomer CE, Hopfer R, McMurray DN, Hickey AJ, “Airways delivery of rifampicin microparticles for the treatment of tuberculosis”. J Antimicrob Chemother, 2001, Vol 48, pp 431-434.
- Suarez S, O’Hara P, Kazantseva M, Newcomer CE, Hopfer R, McMurray DN, Hickey AJ, “Respirable PLGA microspheres containing rifampicin for the treatment of tuberculosis: screening in an infectious disease model” Pharm Res, 2001, Vol 18, pp 1315–1319.
- Alhajlan M, Alhariri M, Omri A, “Efficacy and safety of liposomal clarithromycin and its effect on Pseudomonas aeruginosa virulence factors”. Antimicrob Agents Chemother, 2013, Vol 57, pp 2694-2704.
- d’Angelo I, Conte C, Immacolata La Rotonda M, Miro A, Quaglia F, Ungaro F, “Improving the efficacy of inhaled drugs in cystic fibrosis: Challenges and emerging drug delivery strategies.” Adv Drug Del Rev, 2014, Vol 75, pp 92–111.
- Cheow WS, Chang MW, Hadinoto K, “The roles of lipid in anti-biofilm efficacy of lipid–polymer hybrid nanoparticles encapsulating antibiotics”. Colloids Surf A Physicochem Eng Asp, 2011, Vol 389, pp 158–165.
- “The PreciseInhale™ platform”.
- Ringstad L, “Interaction beteween antimircrobial peptides and phospholipid membranes”. PhD Thesis, Uppsala University, 2009.