Citation: Bibber D, “Scalability of Micro Intraocular Implants and Devices”. ONdrugDelivery Magazine, Issue 63 (Jan 2016), pp 22-24.
Donna Bibber discusses some of these micro-intraocular implants and devices and the scalability challenges associated with each, from the perspective of a plastics engineer.
Recent developments and new-to-market intra-ocular devices and implants have led to the successful treatment of a number of ophthalmological conditions of varying seriousness and complexity such as:
- Glaucoma
- Cataracts
- Retinal detachment
- Diabetic retinopathy
- Age-related macular degeneration
- Uveitis
- Dry-eye syndrome.
Treatment of these conditions often requires collaboration between ophthalmological surgeons, pharmacologists, and micro-specific contract manufacturers. Development of these devices and implants occurs through a large number of highly focused, research-driven specialists, including and micro fabrication specialists, such as:
- Small, innovation-support funding programs
- Development companies that easily find a large marketing partner
- Big pharma funding the outsources of the development instead of doing it in-house.
To design and build scalable intra-ocular implants and devices, the design and fabrication plan must include highly precise, micro sized component made from ultra-thin yet strong materials. These materials must be selected and characterised carefully to be robust enough to last for many years in a moist and warm environment.
In order to scale-up a polymer device that may have been born in an academic or laboratory setting, one must first understand the physical characteristics of the eye (Figure 1) and how the surgeon will be installing the implant or device. The eye is a complex and sensitive organ with many structures and targets located closely together. These some-times conflicting structures have significant defence mechanisms (tear film, cornea) that make it difficult for medication to enter. Vitreous fluid is difficult for injected medication to traverse to the posterior of eye.

Figure 1: Sectional anatomy of the eye (photo credit: visionbesteyecare.com).
When designing and fabricating micro-moulded devices and implants for the human eye, the physical characteristics and material consistency of the components of the eye are critical to understand. Figure 2 summarises the physical characteristics and function of each section of the anatomy of the eye.
The anatomy and physiology of the eye is one of the most complex and unique systems in the human body. Many of these components of the eye are gelatinous, flimsy, easily punctured, and sensitive. As a result, the implants and devices that are installed must be free of sharp edges, excess material or flash, and have absolutely pristine surface finishes to help ensure both surgeon and patient compliance. The instruments, however, which cut or slice into the various components of the eye to install the implants and devices must be very sharp and precisely made to create correctly sized and shaped incisions. Conversely, the instrument to hold or expand the eye open during surgery must be free from parting lines, flash, or sharp edges.

Figure 2: Physical characteristics and functional elements of the eye.
Ophthalmologists are meticulously detailed surgeons with extremely good dexterity and their instruments must match their character traits, as their instruments and implants are considered an extension of meticulously planned and executed procedures. The many layers of the eye require the surgeons to switch quickly and accurately from one instrument to another because of the different surfaces they encounter in the eye.

Figure 3: Sclera Image courtesy of Wikipedia.
US baseball star Yogi Berra once stated: “I’d give my right arm to be ambidextrous.” But having the ability to switch hands and instruments and use both hands during eye surgery enables quick and precise positioning of instruments and safety and efficacy is maintained with instruments designed for the comfort and use in either hand. This requires a look at not only human factors, but also design-for-manufacturability, as the features and tolerances of the device and wall thickness and aspect ratios approach “design challenges” for a particular material selection.
MATERIAL & DESIGN CHARACTERISTICS
Understanding the body’s reaction to polymeric implants is complex. Not only is the natural response affected by the chemical properties of the polymer but also by the physical properties of the implant. Development of an ophthalmologic drug delivery device requires design criteria compatible with the delicate nature of the eye, including proper materials, size, shape, and porosity.
Material Selection
Some materials, although tested for biocompatibility, may still cause inflammation and immuno-responses leading to long term effects on the eye. It is advantageous for safety, regulatory robustness, and speed to market reasons to select not only select a predicate material (PMMA, silicone), but also the predicate grade used in an intraocular application. Families of materials vary greatly from grade to grade in terms of both physical and chemical properties. For example, leachables and extractables over time can vary greatly with different grades of silicone and PMMA and these factors are critical to long term implant and device safety and efficacy. Additional material selection considerations include materials that are slippery , flexible, and non-hydroscopic for compliance adherence.
Size
Ophthalmologic implants or devices must be very small and pliable to fit into the sections of the eye. For example, a glaucoma drain must fit into the sclera which is from 0.3-1.0mm thick (see Figure 3). A part’s thickness and size is dependent on the ocular area and location of the implant, but also chosen on the melt flow of the materials.
Shape
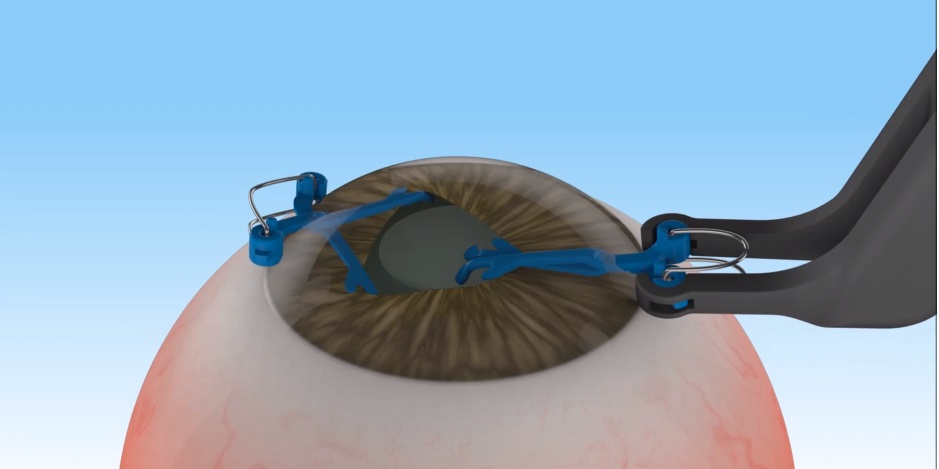
Figure 5 shows a pupil expander device with micro features and surface finishes
necessary to fit comfortably in the eye and provide tensile strength with fine alignment and mechanical strength to hold them in place.
Figure 6 shows a delivery device that sits on the cornea – it’s a thin membrane-like, silicone structure with radial design, and a 50 μm wall thickness to fit inside the upper eyelid. The cornea has 5-6 layers varying from 2-20 μm in thickness, made up of highly sensitive pain receptors. Cornea pain receptor density is up to 600 times that of skin, which is why even a slight injury to the eye is extremely painful.

Figure 4: A polypropylene glaucoma drain.

Figure 5: Pupil-expanding devices
(photo credit: APX Ophthalmology).

Figure 6: Silicone corneal drug delivery device.
Surface Finish/Porosity
In micro-moulded ocular implants and devices, parting lines where the mould’s halves come together, and surface finish of the moulds that create the moulded parts, must meet stringent comfort standards required for them to be worn or implanted. The implications for compliance are clear. Surface finish, blending parting lines, spherical radii, and matching cores and cavities to ultra-precision tolerances (A2 or A1 finishes) are the keys to creating implants that can stand the test of time in an intra-ocular environment.
In the context of an ocular implant, smooth materials can have very different tissue and nerve responses compared with micro-structured materials. Tissue encapsulation of a foreign body (such as the implant) is higher with rougher surfaces because there is more surface area for the implant to attach to tissue. Nerve response to surface finish needs to be considered in implant design. Wear or degradation of a rough surface is more prevalent as well because the smaller porous particles in the surface can be toxic to tissue, can spread throughout the eye, and also trigger an allergic response.
CONCLUSION
The anatomy and physiology of the eye is one of the most complex and unique systems in the human body. Micro-moulding is a scalable process with particular design criteria met, including proper size, three-dimensional shape, wall thickness, material selection, and surface finish.
Micro-injection moulding is a viable and scalable process for fabricating ultra-precise, micro-sized, ultra-thin, yet robust implants and devices located in a highly complex environment such as the eye.
Scalability is an important consideration at the initial product and process design phase in order to achieve the economies of scale – tens, to hundreds of thousands of parts, to millions annually – that micro-moulding offers.
Careful consideration of surface finish, feature size and material selection is paramount to the successful integration of marrying micro-moulding technology with the internal chambers and inter-connective functions of the eye.