To Issue 127
Citation: Norris D, Allen M, Hewson K, Sanchez K, “Waiting for the Outbreath – What Might Covid-19 Bioaerosol Research Have to Tell Us About Inhalable Drug Delivery?”. ONdrugDelivery, Issue 127 (Nov 2021), pp 6–8.
Deborah Norris, Mark Allen, Karl Hewson and Karla Sanchez, discuss how the covid-19 pandemic has spurred research in the pulmonary space, which suggests that a patient-tailored approach based on their individual lung characteristics, facilitated by advanced technology, could improve patient health outcomes and quality of life.
“There is particular interest in the generation of the small aerosol particles that are believed to be generated primarily in the deep lung, at the level of the bronchioles leading to the alveolar sacs – a phenomenon known as ‘bronchiolar fluid film burst’.”
Over the past year-and-a-half living through the covid-19 pandemic, research into the generation and emission of bioaerosols has increased significantly. Studies have looked into the mechanics of how viruses are communicated through respirable droplet production, not just for droplets generated during coughing and sneezing but also during normal breathing and talking.1 Examining these mechanisms has reinforced the existence of “super emitters” – people who produce aerosol particles at an order of magnitude greater than the baseline.2 This research has led to compelling findings.
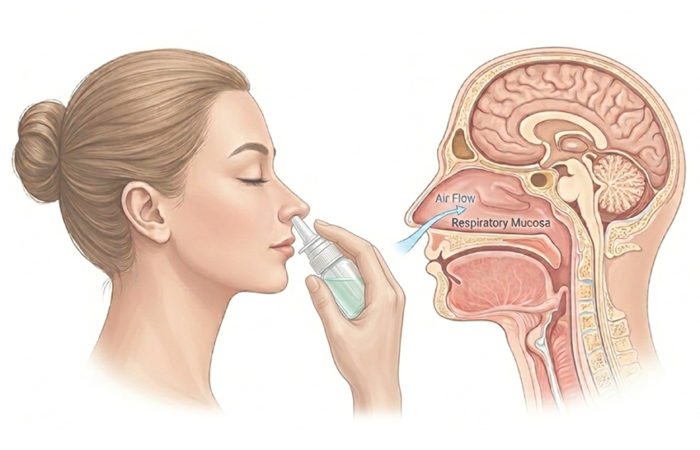
There is particular interest in the generation of the small aerosol particles that are believed to be generated primarily in the deep lung, at the level of the bronchioles leading to the alveolar sacs – a phenomenon known as “bronchiolar fluid film burst”.3 These tiny passages close at the end of a forceful exhalation and re-open as the person inhales, but are covered over by a thin mucosal film – similar to a bubble-wand. This film bursts as inhalation completes, generating microscopic droplets of fluid in the alveolus. Then, during the ensuing exhalation, these tiny particles are ejected from the lung and expelled as an extremely fine bioaerosol.
“The strong exhalation cycle may, in fact, be inhibiting optimal deposition of drug product by encouraging the closure of areas of the lung for targeted medication.”
This is instructive in terms of disease transmission and therefore a hot topic for understanding the communication of bioaerosol-borne viruses. However, it also provokes an interesting discussion around inhaled drug delivery mechanisms. Typically, patients are told to breathe out strongly immediately before administering an inhaler dose. This encourages the patient to achieve the “empty lung” residual volume point and allows for deep inhalation by pulling inhaled medication deeper into the lung. Or does it? Does it, at least, achieve this most effectively? The strong exhalation cycle may, in fact, be inhibiting optimal deposition of drug product by encouraging the closure of areas of the lung for targeted medication. Should we perhaps be looking more closely at understanding and characterising the mechanics of the outbreath to help us improve the efficacy of drug delivery and treatment outcomes?
“By combining traditional diagnostic technologies with cutting-edge techniques to monitor the condition of the lung during the breath cycle, it is possible to open up further potentially exciting developments.”
Studies show that whilst bronchiole closure happens mainly during the deep exhalation stage, age, disease or excess weight can cause this closure point to come at an earlier stage of exhalation, thereby altering bioaerosol emission.4 Could there be room for a patient-specific protocol based on an individual’s lung performance during typical and conscious breathing? This could help healthcare practitioners prescribe patients with inhalers best suited to their physiology – for example, a dry powder, soft mist or pressurised metered dose inhaler, or even a nebuliser – and, in so doing, improve treatment efficacy and possibly adherence too, if the patient feels that they are receiving an enhanced medicinal benefit by using an inhaler that has optimal performance for their breathing patterns.
Devices exist that monitor and analyse patient behaviour in real time during clinical studies and training, such as Cambridge Design Partnership’s Quantii.5 By combining traditional diagnostic technologies with cutting-edge techniques to monitor the condition of the lung during the breath cycle, it is possible to open up further potentially exciting developments. An example is Wheezo (Respiri, Melbourne, Australia), a monitoring tool aimed at helping asthmatics better measure and manage their condition using a connected acoustic device that characterises wheezing episodes.
This highlights the fact that artificial intelligence-based diagnosis devices are no longer the sole preserve of science fiction but a tangible reality. Therefore, the question is how best to use these new insights into outbreath mechanics to develop diagnostics as technology advances. The possibilities include a smart spirometer that can identify the early warning signs of lung conditions; a handheld device that can identify the current health risk for those with lung conditions posed by the environment they are in; and smart-inhaler technology that gathers long-term patterns of a patient’s respiratory profile that, over time, could enable healthcare providers to fine-tune prescriptions and treatment regimens, or even produce on-the-fly adjustments to the applied dose, depending on real-time diagnostic readings at point of care.
Building a picture of an individual’s “lung characteristics” could improve the quality of life and health outcomes for patients with respiratory conditions. Combining advances in artificial intelligence with a deeper understanding of lung mechanics could lead to earlier diagnoses for diseases that are not currently identified before significant structural damage has already occurred. Such a diagnosis could enable healthcare practitioners to offer earlier intervention strategies and a tailored inhaler profile to best match an individual patient’s needs.
Some of these ideas still belong in the field of sci-fi – but there are clearly exciting developments for the respiratory field to pursue, courtesy of research catalysed by the covid-19 pandemic.
REFERENCES
- Pöhlker ML et al, “Respiratory aerosols and droplets in the transmission of infectious diseases”. arXiv:2103.01188, Mar 2021.
- Edwards DA et al, “Inhaling to mitigate exhaled bioaerosols”. Proc Natl Acad Sci USA, Dec 2014, Vol 101(50), pp 17383–17388.
- Johnson GR, Morawska L, “The mechanism of breath aerosol formation “. J Areosol Med Pulm Drug Deliv, 2009, Vol 22(3), pp 229–237.
- Edwards DA et al, “Exhaled aerosol increases with COVID-19 infection, age, and obesity”. Proc Natl Acad Sci USA, 2021, Vol 118(8), Article 2021830118.
- “Quantii: Multi-application sensor platform to analyze patient behaviour”. Company Web Page, Cambridge Design Partnership, Accessed Nov 2021.