
Citation: Wild L, Fuensalida Pantig GR, “The “Customisable Platform” Paradox”. ONdrugDelivery, Issue 113 (Oct 2020), pp 80–85.
Lyndon Wild and Gene Rhode Fuensalida Pantig present a systematic analysis of the customisable platform architecture found in the Molly® autoinjector technology.
The concept of modularity stems from the general attempt to operationalise and understand many complex systems. In 1962, Herbert Simon wrote a paper titled “The Architecture of Complexity”, describing the idea of the near decomposability of many systems – whether it be in social, organisational, physical, chemical or biological constructs. In essence, near decomposability describes the property of systems to be composed of simpler, interacting parts. Then in 1964, Christopher Alexander’s “Notes on the Synthesis of Form” expounds on design thinking and modularity by describing the nature of design problems, the cognitive limits of designers and the modular approach to solving design needs.
In a more recent viewpoint, Martin Sköld’s 2017 book titled “Modularization: The Art of Making More by Using Less” discusses the advantages of applying modularisation in industrial offerings. Modularity, while often ignored, offers double competitiveness to organisations in the form of product cost effectiveness and freedom of customisation.1,2,3
On the other hand, in George Kubler’s “The Shape of Time: Remarks on the History of Things”, the major points of contention also remain relevant to this day, even if we go specifically to the medical device industry. Briefly, Kubler discusses the all-encompassing idea of the creation of objects over time – that the manufacture of art and tools all correspond to a certain need and must pass through the process of design. A tool, however elaborate its mechanisms may be, is always intrinsically simple as a reflection of the specific need it addresses.4
The common denominator here is that the grander scheme of design, not only of intangible things but also of tools, is dependent on a problem that needs a simple, purposeful and cost-effective solution. Interestingly, this concept is still reflected in the science of drug development and delivery. Contingent on patient convenience, healthcare delivery has always suffered low end-user engagement and adherence.5,6 For a long time, administration of parenteral drugs relied on healthcare professionals,7 meaning patients would have to visit their clinics continually to get their medication regimen. Addressing this, the constant development and innovation of patient-operated devices, such as autoinjectors, has enabled self-administration of medicaments in the comfort of one’s home.8
DEFINING THE “CONVENTIONAL PLATFORM” DEVICE
Strictly speaking, there is no textbook definition of what an autoinjector device platform technology is. An extensive NCBI PubMed search using the keyword combinations (autoinjector + platform) or (autoinjector + technology) or (self-injection + platform) would yield a total of only 67 published results.9 However, from these papers, one cannot find an intensive research article or review paper describing details that relate to what an autoinjector platform exactly is.
Nevertheless, it could be said that the current notion about platform devices is attributed to the medical device industry’s idea of what a platform device offering should be. Whilst industry publications have been covering the topic, at present there are very few industry-focused articles in the scientific literature that mention the platform device concept. If we go through the platform-based offerings of various device companies, most of them outline the following qualities:10
- Fast time to develop based on a preconfigured device design
- Availability of common toolsets for device parts, supporting reduced initial costs
- Preset industrial design vetted for various user-group scenarios.
REDEFINING THE PLATFORM MODEL
While there are no universal characteristics of “conventional platforms”, they do share a set of common disadvantages. For instance, a clear-cut trade-off for fast development time entwined with platform devices is the loss or diminishing level of flexibility to device customisations, whether it be in accordance with the customer, primary container, branding or patient requirements. This opens up a myriad of challenges for combination product development – especially when designing for market differentiation or device distinguishability for patients is essential.
Within the last decade, device companies have been tasked to define what a platform device technology should be. These platform devices, ideally, should ultimately address the needs of various stakeholders while delineating patient concerns and mitigating use-related risks. In principle, the most critical points would be the interplay between device design for both manufacturing and end-user requirements. On the pharma side, the design should be distinct for branding purposes, as well as enable optimised manufacturing timelines. For patients, it should enable ease of handling and operation by various patient groups.
When looking at unmet patient needs, the challenges for device offerings in the field of self-injection include polypharmacy, requiring multiple medications,11 and multimorbidity, suffering multiple chronic diseases.12 While there is a definite correlation between polypharmacy and multimorbidity, the patient-use context differs, and the points of contention matter in order to develop an appropriate device.11 In current practice, polypharmacy may involve using the same type of autoinjector device platform across varying dose strengths. Patients suffering from multimorbidity may have more operational challenges while needing to use combination products developed using the same platform device design.10 Patient age group is another important consideration, given the prevalence of chronic diseases is higher in older people. Age is also a relative factor in the ability of users to distinguish a medication or device.10,13
Recent studies indicate the need for self-injection devices that offer a wide range of customisations in line with the intended purpose of each drug delivery device. For example, a 2011 research paper investigated the ability of US patients with diabetes to distinguish between pen injectors based on the same device platform. Interestingly, the researchers found that device differentiation by full pen device colouring, rather than solely label colour, enhances the patient’s ability to differentiate the devices.14 These findings provide insights into the critical importance of autoinjector platforms that offer holistic design adjustments or a completely bespoke industrial design, all the while being enabled by standard internal parts built upon a robust device technology.
THE “CUSTOMISABLE PLATFORM” PARADOX
“The idea of a customisable platform offers a way to leverage the advantages of a platform device technology while still allowing for various customisations in the device design.”
Because design considerations for patient-centric injection systems are multifactorial (i.e. should ideally consider the drug, primary container, industrial design and end-user requirements), design flexibility for conventional, platform-based devices is delimited; a platform device that does not offer discrete and defined sets of customisations will always result in a similar resultant product. This raises concerns in combination product development.
The idea of a customisable platform offers a way to leverage the advantages of a platform device technology while still allowing for various customisations in the device design. Although paradoxical, a customisable platform offering exists. The lens of mathematics offers us a way to illustrate the idea and logical validity of customisable platforms. In the case of SHL’s Molly®, its modularisation enables a robust core technology that allows bespoke customisations in the front and rear sub-assemblies of discrete device projects.
In combinatorics, the customisable platform could be best illustrated, and likewise proofed, using set theory and pi notation (Figure 1), allowing us to demonstrate the extent of possible device customisations using modular design.
From this, we can generalise that the number of customised devices that could be developed based on Molly® is finitely large. This level of freedom is truly important when considering the various needs of stakeholders in combination product development.

Figure 1: Using a combinatorics approach, set theory and pi notation allow us to demonstrate the extent of device customisations enabled by modular device design.
MODULARITY BUILT UPON A PLATFORM
The “double competitiveness” put forth by Martin Sköld3 is reflected in Molly’s flexible design and development model. Through building a platform device technology supported by similarly modular manufacturing streams, pharma partners are presented with cost-effective options for their combination product projects.15
The key point here is that a platform does not need to be modular – but modularity is something that is built upon a platform. Hence, it is the well-established Molly® platform device technology that allows SHL to build modularity upon the device sub-assemblies. Interestingly, this modularity extends to various layers of the device development process, where several device testing and assembly infrastructures that SHL uses are, in a sense, modular.15 In doing so, SHL creates a duality in the advantages of its Molly® offering – cost effectiveness in device manufacturing as well as customisations in the device design.
A ROBUST DEVICE DESIGN ENABLED BY MODULAR COMPONENTS
With little empirical evidence for the distinguishability of lookalike autoinjectors among users, patient handheld devices based on the same technology must enable design customisations for differentiation.10,14 Using a retrospective analysis of Molly® device projects (Figure 3), it could be reasoned that the maturity of the preconfigured platform device model has enabled the customisations found in subsequent Molly® bespoke projects. Of important note is that both the 1.0 mL and 2.25 mL standard versions of the Molly autoinjector reflect a modular approach in their core design technology.

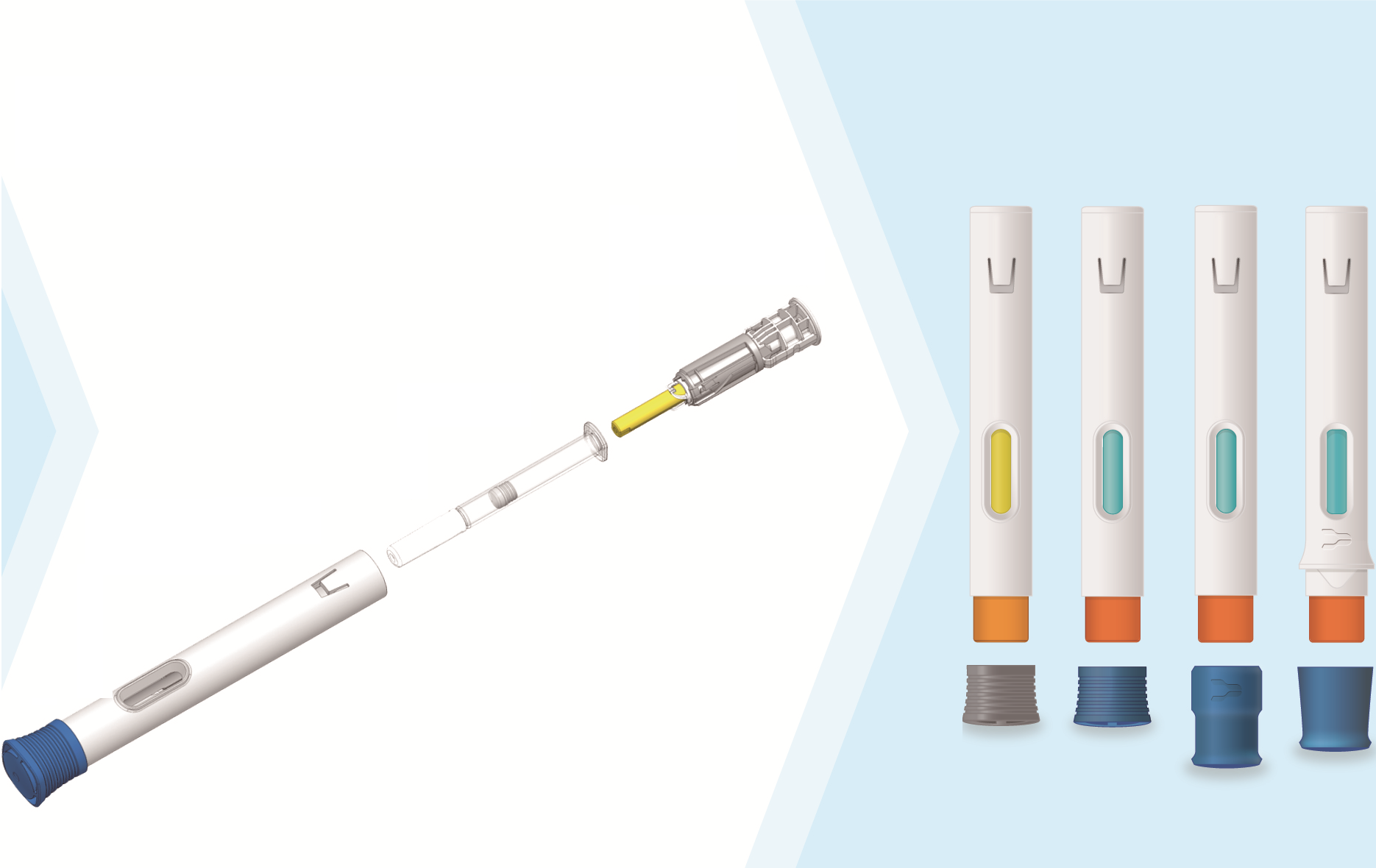
Figure 2: Standard modular components along with the customisable parts of the Molly® platform technology, giving rise to finitely many device configurations of varying colours and geometries (device renderings are not representative of any final offering).
For instance, the Molly® device technology is modular in the sense that both the front and rear sub-assemblies comprise five to six intricately designed parts. This preconfigured technology allows an appreciable level of freedom for customisation while maintaining its rotator-based mechanism (Figure 2). With front and rear modules comprising its integral components, Molly enables design feature modifications to differentiate a device’s appearance. For instance, the colour of the cap, needle cover and plunger rod can be changed. Aside from these, device body customisations, not only for branding and market differentiation but also for patient distinguishability and usability, are possible; for Molly device projects, the core technology components always remain intact while a degree of customisation may be seen in its industrial design.
BESPOKE PROJECTS USING A CUSTOMISABLE PLATFORM
Looking at the commercialised Molly® device projects in the past, we truly see the competitive advantage of a modular platform. A bidirectional comparison of each commercialised device highlights Molly’s flexibility in industrial design.
In Figure 3, the industrial design of device A compared with device B shows a stark difference in design but reflects the level of flexibility afforded by a customisable platform technology. This difference could be viewed in terms of the requirements of the drug, patients’ disease state and user-group handling needs, among others. On the other hand, device D highlights how Molly® can support lifecycle management, wherein the prefilled syringe and complex biologic have been co-developed in two device versions for varying dosing needs.

Figure 3: Commercialised projects based on the customisable Molly® platform.
It is interesting to note that these device projects were initiated on independent timelines, highlighting the robustness of the Molly® platform over time. Such a modular platform allows for bespoke offerings to every customer, supported by a design and manufacturing model that can be scaled according to the purpose and demands of production. Finally, the idea of bespoke device projects based on the Molly technology is further substantiated if we do a non-exhaustive but multisource survey and comparison of commercially available platform-based autoinjectors.10,16
It could be said that, alongside these, experience with Molly® projects translates into the parallel maturity of infrastructures that support the design and development ecosystem of such device projects. With a device technology built upon standard modules and mature infrastructures, Molly® supports customised solutions according to a drug, pharma and patient’s requirements.
THE BENEFITS OF A CUSTOMISABLE PLATFORM
Across various industries, the benefits associated with customisable platforms are manifold. In our day-to-day lives, we encounter numerous examples of products built on these principles, including cars (Volkswagen), power tools (Black & Decker) and printers (Hewlett-Packard’s Deskjet). Although these examples are drawn from very diverse industries and applications, they share many key common fundamentals (e.g. built on robust core technology, scalable for high-volume manufacture, customisable, speed to market and cost optimised).17,18,19,20
These key drivers exemplify why so many everyday products are designed and built using customisable platform technologies; they are also relevant and completely applicable to autoinjectors. SHL understands that customisation should not be an option but an inherent property that extends according to project needs. Hence, the Molly® technology combines the advantages of modularisation and platform, allowing us to establish a flexible design and development model (Figure 4). To do this, SHL uses the commonality of a platform, allowing us to share manufacturing assets across Molly device projects. Although not without its risks, the reliability brought about by an established platform supports the simplification of project processes and optimisation of timelines.

Figure 4: A customisable platform that is found in Molly®. Full device representations resulting from various customised device attributes chosen from among the customisable parameters of the Molly® device (device renderings are not representative of any final offering).
CONCLUSION
In SHL’s February 2020 ONdrugDelivery article,21 we reinforced the need for an even tighter collaboration from drug research through to the development of combination products.10 To do so would mean that a device design could address the ever-changing needs within the continuum of drug-device development.
While not yet a norm, the industry as a whole should move away from platform products and towards developing platform technologies – giving rise to flexible device offerings that address the unmet needs in drug delivery systems. At present, Molly® has been embodied in multiple commercial launches, addressing various disease areas. This highlights the stratification of device offerings in the market and puts the Molly technology in a unique position.
SHL believes that the future of devices will be mass customisation. To support the maturity of its pipeline and commercialised projects, lifecycle management is a key driver that the Molly® customisable platform is designed to address. The true value of Molly® lies in its flexible design and development model that will continue to scale in response to industry advances, such as in data science and future device add-ons that live within a reformulated digital health ecosystem.22,23
REFERENCES
- Simon H, “The Architecture of Complexity”. Proc Am Philos Soc, 1962, Vol 106(6), pp 467–482.
- Alexander C, “Notes on the Synthesis of Form”. Harvard University Press, 1964.
- Sköld M, “Modularization: The Art of Making More by Using Less”. Rheologica AB, 2017.
- Kubler G, “The Shape of Time: Remarks on the History of Things”. Yale University Press, 1962.
- Jin J et al, “Factors Affecting Therapeutic Compliance: A Review From the Patient’s Perspective”. Ther Clin Risk Manag, 2008, Vol 4(1), pp 269–286.
- Hugtenburg J et al, “Definitions, Variants, and Causes of Nonadherence With Medication: A Challenge for Tailored Interventions”. Patient Prefer Adherence, 2013, Vol 7, pp 675–682.
- Maniadakis N et al, “A Targeted Literature Review Examining Biologic Therapy Compliance and Persistence in Chronic Inflammatory Disease to Identify the Associated Unmet Needs, Driving Factors, and Consequences”. Adv Ther, 2018, Vol 35(9), pp 1333–1355.
- Gurman P et al, “Prefilled Devices for Parenteral Applications”. Expert Rev Med Devices, 2014, Vol 11(2), pp 205–223.
- NCBI Resource Coordinators, “Database Resources of the National Center for Biotechnology Information”. Nucleic Acids Res, 2019, Vol 47(D1) pp D23–D28.
- ONdrugDelivery, Issue 105, (Feb 2020) pp 8–12.
- Masnoon N et al, “What Is Polypharmacy? A Systematic Review of Definitions”. BMC Geriatr, 2017, Vol 17(1), pp 230.
- Marengoni A et al, “ Aging With Multimorbidity: A Systematic Review of the Literature”. Ageing Res Rev, 2011, Vol 10(4), pp 430–439.
- Hajat C, Stein E, “The Global Burden of Multiple Chronic Conditions: A Narrative Review”. Prev Med Rep, 2018, Vol 12, pp 284–293.
- Lefkowitz M, “Do Different Body Colors and Labels of Insulin Pens Enhance a Patient’s Ability to Correctly Identify Pens for Injecting Long-Acting Versus Short-Acting Insulins?” J Diabetes Sci Technol, 2011, Vol 5(1), pp 136–49.
- Fluetsch G, Chung L, “Expanding Automation Capacity for High and Low Volumes”. ONdrugDelivery, Issue 99 (Aug 2019), pp 6–9.
- Pharmacircle, 2020.
- Meyer M, Utterback J, “The Product Family and the Dynamics of Core Capability”. International Center for Research on the Management of Technology, Sloan School of Management, Massachusetts Institute of Technology, 1992.
- Sköld M, Karlsson C, “Product Platform Development in Industrial Networks”. Int J Automotive Technology and Management, Vol 11(3), pp 205–220.
- Gawer A, Cusumano M, “Platform Leadership: How Intel, Microsoft, and Cisco Drive Industry Innovation”. Harvard Business School Press, 2002.
- Meyer M, Lehnerd A, “The Power of Product Platforms: Building Value and Cost Leadership”. Free Press, 1997.
- Fuensalida Pantig GR, “Addressing complex biologics with rational drug device design”. ONdrugDelivery, Issue 105, (Feb 2020) pp 8–12.
- Gertz F, Fleutsch G, “Applications of Deep Learning in Medical Device Manufacturing”. ONdrugDelivery, Issue 110 (Aug 2020), pp 6–11.
- Williams C, Rafiei R, Howald R, “Digital Health Reformulation: from Hope to Hype to Health”. ONdrugDelivery, Issue 108 (June 2020), pp 51–56.
